Assessing Otitis Externa in the Dog
Assessing Otitis Externa in the Dog
Successful management of canine otitis externa requires:
- Complete assessment of the outer ear and ear canal
- Appropriate diagnostics to identify primary and secondary conditions
- An understanding of these conditions
- Knowledge of available topical therapies for treatment and management
This step-by-step guide was developed by Dr. Russell Muse, DVM, DACVD, MANZCVS. He will lead you through some of the common decisions involved in identifying the type of ear disease, interpretation of diagnostics, and suggestions for therapy and management.
Is the ear inflamed?


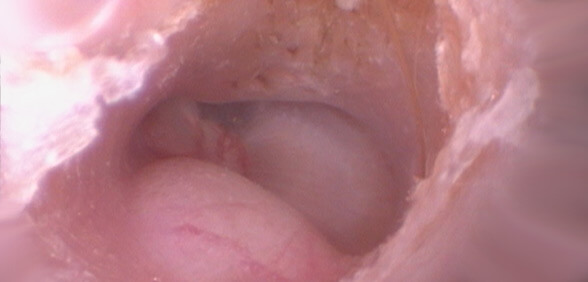
Can you visualize the horizontal canal with a hand-held otoscope?
Can you place your otoscope head into the patient’s ear with relative ease and without causing significant objection or pain?


Can you visualize the tympanic membrane?

Is discharge present in the canal?
When you evaluate the ear canal, does significant discharge in the canal partially or fully obstruct your view of the tympanic membrane?


After steroid administration, can you now visualize the horizontal canal?
Is discharge present in the canal?
When you evaluate the ear canal, does significant discharge in the canal partially or fully obstruct your view of the tympanic membrane?
Does the canal have proliferative tissue?

What does cytology show?
Administer five to seven days of steroids (if appropriate for the patient)
If not, consider sedation for improved visualization.
Consider sedation/anesthesia or referral for video-otoscopy or other imaging
Video-otoscopy can be an important tool for dogs with chronic or recurrent otitis externa that may also have otitis media. Video-otoscopy procedures allow for improved visualization of the deeper horizontal canal and tympanic membrane. They also enhance cleaning ability and removal of all remnants of infection. CT scans can also be helpful in evaluating potential middle ear disease, the bony aspects of the middle ear, and calcification of the outer ear. This evaluation can assist you in deciding whether medical or surgical therapy is the best option.
Suggestive of ceruminous gland hyperplasia or neoplasia
Ceruminous gland hyperplasia
The presence of ceruminous gland hyperplasia in the ear canals generally indicates chronicity with structural changes further complicating otitis management. However, some cases may develop in the absence of obvious chronic infection because of the intermittent presence of subtle inflammation or bacteria in the ear canals. Both occur commonly in allergic otitis. Chronic inflammation in atopic skin leads to epidermal thickening and dermal inflammation leads to infiltrates, edema, or fibrosis and increased dermal thickness. As the skin thickens, varying degrees of ear canal stenosis will result. At this point, altered epithelial migration, a perpetuating factor, is most often present. In addition to these changes, failure of epithelial migration will lead to more exudate and debris filling the ear canal. The exudate, inflammation, possible aggravated allergic response, and epidermal damage are additional perpetuating factors, which eventually become the main factors in the worsening OE.
Inflammation changes adnexal structures as well and histopathologic studies on OE cases reveal varying degrees of fibrosis, sebaceous gland hyperplasia, and ceruminous gland (apocrine gland) secretion-filled dilation and hidradenitis (pustular nodules). Thickened tissue often results in keratinous-filled epithelial folds, which may occlude glandular and follicular ostia. Once perpetuating factors occur and become severe enough, otitis externa continues or recurs even if the causes are resolved. These perpetuating factors also promote resistant or recurrent infection and the keratin can become a biofilm substrate.
Treatment for these conditions includes reduction of the ceruminous hyperplasia and discharge with oral corticosteroids or even long-term cyclosporine administration. Additional modalities include adequate evaluation and cleaning of the canal through video otoscopy if possible, and in cases of chronicity, computed tomography evaluation to determine the degree of disease of the middle ear.

Neoplasia
The presence of a mass in the ear canal can be straightforward, or in other cases, more problematic. An obvious mass in the ear canal that can be visualized with a handheld otoscope creates no difficulty in diagnosis. Inflammatory polyps can be found in dogs and may be removed via manual extraction in some cases and video otoscopy or surgical intervention in others. If the polyps can be successfully removed, then the infection can generally be resolved if no significant chronic changes are noted.
However, other cases of neoplasia can be more difficult to diagnose because of ear canal inflammation or the presence of infection, discharge, or hemorrhage obscuring the mass. In cases of unilateral otitis in an older dog, neoplasia should be suspected. In cases in which a canal cannot be thoroughly evaluated, anesthesia for further investigation should be considered sooner rather than later. Video otoscopy allows for a more complete canal visualization, debris removal, and potential mass removal or biopsy to determine the need for further surgical management. In addition, magnetic resonance imaging should also be considered to determine if the mass has extended into surrounding tissue before performing video otoscopy.
Suggestive of an allergic ear
Allergic otitis is very common in atopic dogs. Typically, inflammation of the medial pinnae and ear canals is observed. Long-term management of the atopic dermatitis is essential to prevent repeated episodes of otitis and infection. In some dogs, the overall management of the atopic dermatitis with oclacitinib, lokivetmab, cyclosporine, prednisolone, or immunotherapy will control the otitis. In other dogs, some additional localized treatment is required to manage and prevent recurrences. This usually involves a once or twice weekly application of a topical glucocorticoid. The use or requirement of additional antimicrobial ingredients should be evaluated in individual situations. Chronic use of topical antimicrobials may lead to more resistant strains of organisms and the risks versus benefits should be considered.
In addition, appropriate and routine cleaning with cleansers designed to eliminate wax and skin cells is important in controlling the environment of the ear canal that promotes infection. Other cleansers that specifically target bacteria or yeasts may also be necessary to discourage overgrowth of these infection-causing organisms in the allergic ear. Each ear is different and appropriate cytology looking for evidence of keratinocytes, bacteria, and yeasts is important in deciding which ear cleansers are right for each individual patient.
Coccoid Bacteria
Given that coccoid bacteria are a normal resident of the ear canal, small numbers seen on cytology can be a normal finding. However, in allergic ears that lose the self-cleaning mechanism with subsequent cerumen and debris buildup, bacterial overgrowth can lead to colonization of the canal with Staphylococcus pseudintermedius and increased levels of pruritus. The goal of managing an allergic ear predisposed to coccoid bacterial overgrowth is two-pronged: treatment aimed at coccoid bacteria and a cleaning regimen addressing the inflammation and character and amount of the discharge in the canal. These factors will dictate the type of cleaner and frequency required.
Treatment with a topical product such as Osurnia® (florfenicol, terbinafine, betamethasone acetate) is an effective therapy for cases of allergic otitis externa with coccoid bacterial overgrowth suspected to be Staphylococcus pseudintermedius. Osurnia® contains florfenicol which has excellent spectrum of activity against most strains of Staphylococcus pseudintermedius. In addition, it contains betamethasone which is a potent steroid and would be a good choice for cases with moderate to severe inflammation of the canal. And because Osurnia® is a repositol gel formulation, frequent manipulation of the ear canal is not necessary in patients with painful ears. Osurnia® should be applied weekly for two treatments. Clean and dry the ear canal before administering the initial dose. Osurnia® is effective for 45 days after the initial treatment, so avoid cleaning during this period to allow contact of the gel with the ear canal.
Topical therapy with Mometavet® (gentamicin sulfate, mometasone furoate anhydrous, and clotrimazole otic suspension) is also effective for susceptible strains of coagulase-positive staphylococci. In addition, it contains mometasone, which is a moderate potency steroid for cases of mild to moderate inflammation of the ear canal.
Topical treatment with Animax® Ointment (nystatin, neomycin sulfate, thiostrepton, triamcinolone acetonide ointment) is also effective for certain strains of coccoid bacteria. In addition, it contains triamcinolone, which is a moderate potency steroid for cases of mild to moderate inflammation of the canal. Animax® Ointment can be an option in cases with coccoid bacteria and mild to moderate erythema.
Cleaning regimens for cases of otitis externa with coccoid bacterial overgrowth should address the inflammation and organisms observed on cytology. Ear cleaners should be used at home as part of most treatment protocols, especially for chronic otitis. Removing debris and discharge improves the efficacy of topical antimicrobials. Depending on the severity of the otitis and amount of discharge present, ear cleaners can be used initially once daily to twice weekly. After the inflammation and infection have resolved, ears are usually cleaned once to twice weekly. Maintenance cleaning dramatically decreases the recurrence of otitis and clients will be more likely to detect a new ear infection earlier.
IMPORTANT SAFETY INFORMATION
As with all drugs, side effects may occur. In field studies and post-approval experience the most common side effects reported were vomiting, increased liver enzymes and loss of hearing. Other signs reported were ear discharge, ear irritation and pain, vomiting, head shaking, head tilt, ataxia, vocalization, corneal ulcer, keratoconjunctivitis sicca, nystagmus, tympanic rupture, and facial paralysis.
Osurnia® should be administered by a veterinary professional. Do not use in dogs with known tympanic perforation or a hypersensitivity to florfenicol, terbinafine or corticosteroids. Osurnia® may cause eye injury and irritation. Wear eye protection when administering Osurnia® and restrain the dog to minimize post-application head shaking. Do not use in cats. Refer to the prescribing information for complete details or visit www.dechra-us.com.
IMPORTANT SAFETY INFORMATION
As with all drugs, side effects may occur. Mometavet® Otic Suspension should be discontinued if hypersensitivity to any component occurs. Concomitant use of drugs known to induce ototoxicity should be avoided. Do not use in dogs with known perforation of eardrums. If hearing or vestibular dysfunction is noted during treatment, discontinue use immediately and flush the ear canal with a non-ototoxic solution. Refer to the prescribing information for complete details or visit www.dechra-us.com.
IMPORTANT SAFETY INFORMATION
As with all drugs, side effects may occur. Hearing loss, with varying degrees of recovery, has been reported with the use of ANIMAX® Ointment. If hearing dysfunction is noted during the course of the treatment with ANIMAX® Ointment, discontinue its use. SAP and SGPT (ALT) enzyme elevations, polydipsia and polyuria, vomiting and diarrhea (occasionally bloody) have been observed following parenteral or systemic use of synthetic corticosteroids in dogs. Cushing’s syndrome has been reported in association with prolonged or repeated steroid therapy in dogs. Refer to the prescribing information for complete details or visit www.dechra-us.com.
240362A
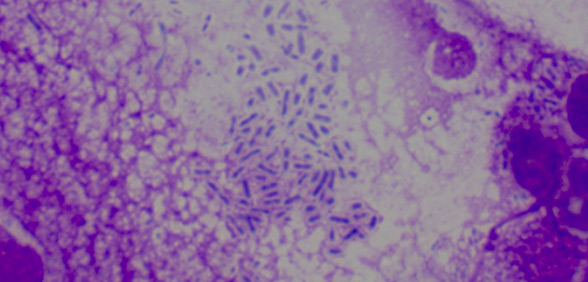
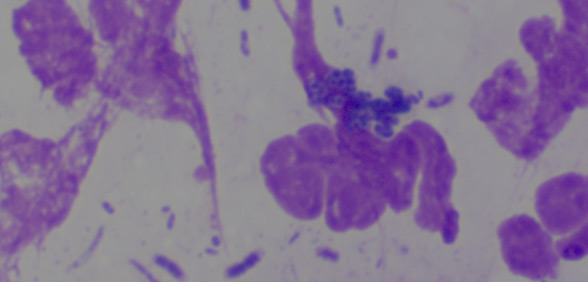
Rod-shaped Bacteria
Rod-shaped bacteria (Proteus, E. coli, and Pseudomonas) are not normal residents of the ear canal and are generally considered opportunistic infections. They can result from contamination of an ear canal that is inflamed or chronically infected with other resident organisms. When these organisms are seen alone or in combination with other infectious organisms, culture should be considered because sensitivities for rod-shaped bacteria can be unpredictable. Allergic ears often lose the self-cleaning mechanism with subsequent cerumen and debris buildup and chronic coccoid bacterial overgrowth; they can then be particularly susceptible to opportunistic organism contamination. These organisms often cause severe pain, with erosion or ulceration of the canal, and substantial discharge. The goal of managing an allergic ear with opportunistic rod-shaped infection involves treatment aimed at the type of bacteria and degree of inflammation as well as a cleaning regimen that considers the amount of inflammation and pain and the character and amount of discharge.
Treatment with a topical product such as Mometavet® (gentamicin sulfate, mometasone furoate anhydrous, and clotrimazole otic suspension) is effective for susceptible strains of Gram-negative rod bacteria, including Proteus and Pseudomonas. In addition, it contains mometasone, which is a moderate potency steroid for cases of mild to moderate inflammation of the ear canal. However, oral steroids may be indicated for significant inflammation. Mometavet® can be an option in cases with rod-shaped bacteria and mild to moderate inflammation while awaiting culture results.
Topical treatment with Animax® Ointment (nystatin, neomycin sulfate, thiostrepton, triamcinolone acetonide ointment) is also effective for certain strains of Gram-negative rod bacteria. In addition, it contains triamcinolone, which is a moderate potency steroid for cases of mild to moderate inflammation of the canal. However, oral steroids may be indicated for significant inflammation. Animax® Ointment can be an option in cases with rod-shaped bacteria and mild to moderate inflammation while awaiting culture results.
Cleaning regimens for cases of otitis externa complicated by rod-shaped bacterial infection should address the inflammation and organisms observed on cytology. Ear cleaners should be used at home as part of most treatment protocols, especially for chronic otitis. Removing debris and discharge improves the efficacy of topical antimicrobials. Depending on the severity of the otitis and amount of discharge present, ear cleaners can be used initially once daily to twice weekly. After the inflammation and infection have resolved, ears are usually cleaned once to twice weekly. Maintenance cleaning dramatically decreases the recurrence of otitis and clients will be more likely to detect a new ear infection earlier.
IMPORTANT SAFETY INFORMATION
As with all drugs, side effects may occur. Mometavet® Otic Suspension should be discontinued if hypersensitivity to any component occurs. Concomitant use of drugs known to induce ototoxicity should be avoided. Do not use in dogs with known perforation of eardrums. If hearing or vestibular dysfunction is noted during treatment, discontinue use immediately and flush the ear canal with a non-ototoxic solution. Refer to the prescribing information for complete details or visit www.dechra-us.com.
IMPORTANT SAFETY INFORMATION
As with all drugs, side effects may occur. Hearing loss, with varying degrees of recovery, has been reported with the use of ANIMAX® Ointment. If hearing dysfunction is noted during the course of the treatment with ANIMAX® Ointment, discontinue its use. SAP and SGPT (ALT) enzyme elevations, polydipsia and polyuria, vomiting and diarrhea (occasionally bloody) have been observed following parenteral or systemic use of synthetic corticosteroids in dogs. Cushing’s syndrome has been reported in association with prolonged or repeated steroid therapy in dogs. Refer to the prescribing information for complete details or visit www.dechra-us.com.
240362B
Mixed Infection
Mixed infections can occur in many chronically infected ears. The normal resident organisms including Staphylococcus pseudintermedius will generally be present and in many cases, contaminant Gram-negative rods will also be present in significant numbers. Rod-shaped bacteria, including Proteus, E. coli and Pseudomonas, are not normal residents of the ear canal. They are generally considered opportunistic infections, resulting from contamination of an ear canal that is inflamed or chronically infected with Staphylococcus. When these organisms are seen in combination, culture should be considered because sensitivities for rod-shaped bacteria can be unpredictable. Allergic ears often lose the self-cleaning mechanism with subsequent cerumen and debris buildup and chronic coccoid bacterial overgrowth; they can then be particularly susceptible to opportunistic organism contamination. Gram-negative organisms often cause severe pain, with erosion or ulceration of the canal, and substantial discharge. The goal of managing an allergic ear with a mixed infection involves treatment aimed at all types of bacteria and the degree of inflammation as well as a cleaning regimen that considers the amount of inflammation and pain and the character and amount of the discharge.
Topical therapy with Mometavet® (gentamicin sulfate, mometasone furoate anhydrous, and clotrimazole otic suspension) is effective for susceptible strains of coagulase-positive staphylococci and Gram-negative rod bacteria, including Proteus and Pseudomonas. In addition, it contains mometasone, which is a moderate potency steroid for cases of mild to moderate inflammation of the ear canal. However, oral steroids may be indicated for significant inflammation. Mometavet® can be an option in cases with rod-shaped bacteria and mild to moderate inflammation while awaiting culture results.
Topical treatment with Animax® Ointment (nystatin, neomycin sulfate, thiostrepton, triamcinolone acetonide ointment) is also effective for certain strains of Gram-negative rod bacteria as well as some strains of coccoid bacteria. In addition, it contains triamcinolone, which is a moderate potency steroid appropriate for cases of mild to moderate inflammation of the canal. However, oral steroids may be indicated for significant inflammation. Animax® Ointment is an option for cases with rod-shaped bacteria and mild to moderate erythema while awaiting culture results.
Cleaning regimens for cases of otitis externa complicated by mixed infections should be directed at the inflammation and the organisms observed on cytology. Ear cleaners should be used at home as part of most treatment protocols, especially for chronic otitis. Removing debris and discharge improves the efficacy of topical antimicrobials. Depending on the severity of the otitis and amount of discharge present, ear cleaners can be used initially once daily to twice weekly. After the inflammation and infection have resolved, ears are usually cleaned once to twice weekly. Maintenance cleaning dramatically decreases the recurrence of otitis and clients will be more likely to detect a new ear infection earlier.
IMPORTANT SAFETY INFORMATION
As with all drugs, side effects may occur. Mometavet® Otic Suspension should be discontinued if hypersensitivity to any component occurs. Concomitant use of drugs known to induce ototoxicity should be avoided. Do not use in dogs with known perforation of eardrums. If hearing or vestibular dysfunction is noted during treatment, discontinue use immediately and flush the ear canal with a non-ototoxic solution. Refer to the prescribing information for complete details or visit www.dechra-us.com.
IMPORTANT SAFETY INFORMATION
As with all drugs, side effects may occur. Hearing loss, with varying degrees of recovery, has been reported with the use of ANIMAX® Ointment. If hearing dysfunction is noted during the course of the treatment with ANIMAX® Ointment, discontinue its use. SAP and SGPT (ALT) enzyme elevations, polydipsia and polyuria, vomiting and diarrhea (occasionally bloody) have been observed following parenteral or systemic use of synthetic corticosteroids in dogs. Cushing’s syndrome has been reported in association with prolonged or repeated steroid therapy in dogs. Refer to the prescribing information for complete details or visit www.dechra-us.com.
240362D
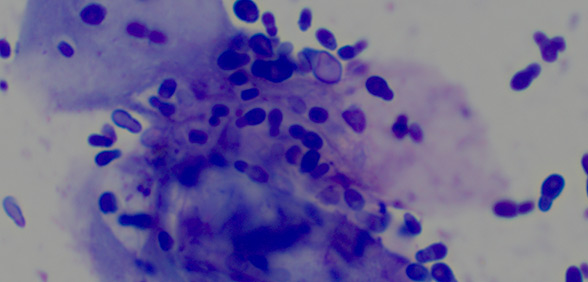
Yeast Overgrowth
Given that yeasts (specifically Malassezia pachydermatis) are normal residents of the ear canal, small numbers seen on cytology can be a normal presentation. However, in allergic ears that lose the self-cleaning mechanism with subsequent cerumen and debris buildup, Malassezia overgrowth can lead to colonization of the canal with these organisms and increased levels of pruritus. Hypersensitivity type reactions can also occur with Malassezia, resulting in exaggerated pruritus when even small numbers are present. The goal of managing an allergic ear with the potential for Malassezia overgrowth involves treatment aimed at these organisms and a cleaning regimen that considers the amount of inflammation and the character and amount of the discharge. This will dictate the type of cleaner and frequency required.
Treatment with a topical product such as DuOtic® (terbinafine and betamethasone acetate otic gel) is an effective therapy for cases of allergic otitis externa with Malassezia overgrowth. DuOtic® contains terbinafine, which has excellent spectrum of activity against Malassezia pachydermatis. In addition, it contains betamethasone, which is a potent steroid and good choice for cases of moderate to severe inflammation. And because DuOtic® is a repositol gel formulation, frequent manipulation of the ear canal is not necessary in patients with painful ears. DuOtic® should be applied weekly for two treatments. Clean and dry the ear canal before administering the initial dose. DuOtic® is effective for 45 days after the initial treatment, so avoid cleaning during this period to allow contact of the gel with the ear canal.
Cleaning regimens for cases of otitis externa complicated by Malassezia overgrowth should be directed at the inflammation and the organisms observed on cytology. Ear cleaners should be used at home as part of most treatment protocols, especially for chronic otitis. Removing debris and discharge improves the efficacy of topical antimicrobials. Depending on the severity of the otitis and amount of discharge present, ear cleaners can be used initially once daily to twice weekly. After the inflammation and infection have resolved, ears are usually cleaned once to twice weekly. Maintenance cleaning dramatically decreases the recurrence of otitis and clients will be more likely to detect a new ear infection earlier.
IMPORTANT SAFETY INFORMATION
As with all drugs, side effects may occur. For Otic Use in Dogs Only. Do not use in cats. Do not use in dogs with known tympanic perforation. Do not use in dogs with a hypersensitivity to terbinafine or corticosteroids. Do not administer orally. Use with caution in dogs with impaired hepatic function. In a field study and post-approval experience following the use of a similar product Osurnia® (florfenicol, terbinafine, betamethasone acetate) the most common adverse reactions were elevated alanine aminotransferase, conjunctivitis, ocular discharge, ear pruritus, deafness, ear discharge, pinnal irritation and ear pain, emesis, head shaking, internal ear disorder (head tilt and vestibular), ataxia, vocalization, corneal ulcer, keratoconjunctivitis sicca, nystagmus, tympanic rupture, and cranial nerve disorder (facial paralysis). The safe use of DuOtic® has not been evaluated in dogs that are pregnant, lactating or intended for breeding. DuOtic® may cause eye injury and irritation. DuOtic® should be administered by a veterinary professional. Wear eye protection when administering DuOtic® and restrain the dog to minimize post- application head shaking. Refer to the prescribing information for complete details or visit www.dechra-us.com.
240362C
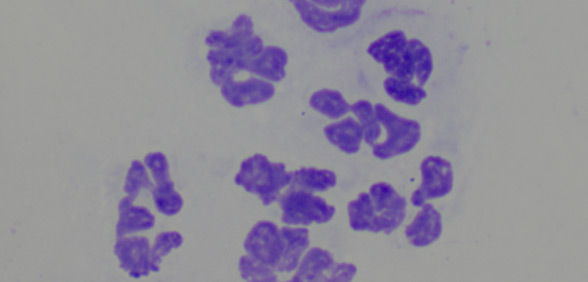
Neutrophils
The presence of neutrophils in the ear canal is pathognomonic for either significant inflammation or infection. Neutrophils in the absence of cytological evidence of infection can either mean that infection is deeper in the ear canal or is within the walls of the canal, or ongoing inflammation is occurring from other primary OE triggers.
Culture and sensitivity should be undertaken to detect low numbers of bacterial organisms. Sedation or anesthesia for a more thorough assessment of the outer ear canal should be considered. Video otoscopy may also be an invaluable tool to more deeply and thoroughly evaluate the canal.
A short course (three to seven days) of oral corticosteroids should be considered to decrease inflammation if appropriate in the individual patient; this should be followed by a recheck.
Treatment needs to be directed at the infection and inflammation. (See the other categories of therapy for coccoid bacteria, rod-shaped bacteria, mixed infection, or yeast infection for recommendations on ear cleaning.)
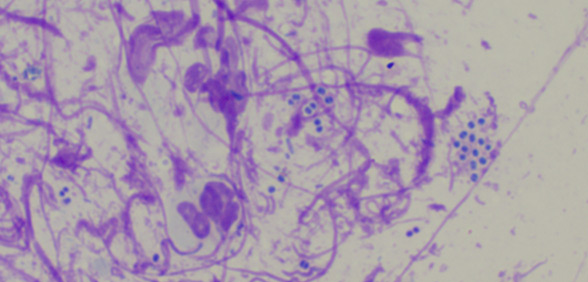
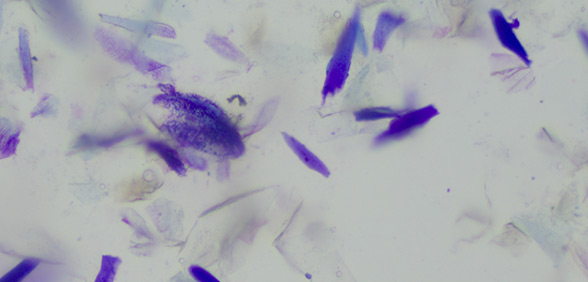
Keratinocytes
Accumulation of excessive keratinocytes or lipid (wax) in the ear canal may result from failure of the self-cleaning mechanism. The orderly migration of keratinocytes and lipids from the lower ear canal and eventually out of the ear is impaired in allergic ears. This migration removes normal organisms and prevents chronic recurrent infection of the ear canals.
Management depends on the nature and character of the build-up. Ear cleaners should be used at home as part of most treatment protocols, especially for chronic otitis. Removing debris and discharge improves the efficacy of topical antimicrobials. Depending on the severity of the otitis and amount of discharge present, ear cleaners can be used initially once daily to twice weekly. After the inflammation and infection have resolved, ears are usually cleaned once to twice weekly. Maintenance cleaning dramatically decreases the recurrence of otitis and clients will be more likely to detect a new ear infection earlier.